

Scolioscan, the world’s pioneering 3D ultrasound-based scoliosis assessment system, generates a true-to-life image of the spine by constructing a three-dimensional spinal model. By utilizing ultrasound technology and innovative software, it accurately captures spinal curvatures. As an excellent alternative to traditional radiography, Scolioscan enables scoliosis evaluation using three-dimensional ultrasound projections. Notably, it operates without the need for a darkened room; the examination takes place under normal lighting conditions, ensuring patient comfort and security. Furthermore, its safety profile allows for repeated use during therapy sessions.
–Sandra Trzcińska Orthopaedic Rehabilitation Centre for Children and Adolescents in Chylice Mazowieckie Rehabilitation Centre
About MAZOWIECKIE CENTRUM REHABILITACJI STOCER
MAZOWIECKIE CENTRUM REHABILITACJI STOCER, located in Konstancin-Jeziorna, Mazowieckie, Poland, operates within the General Medical and Surgical Hospitals Industry. This esteemed rehabilitation center specializes in providing orthopedic services, focusing on the treatment of posture defects and lateral curvatures of the spine in children and adolescents.
![]()

Their Pain Point and our Solution
(1) Actual image of the spine
Existing non-invasive devices employed for scoliosis assessment typically rely on estimated data, derived from body surface measurements. These images serve as illustrations, lacking precision. In contrast, the Scolioscan device surpasses this limitation by producing actual images during assessments without the need for invasive procedures. A comprehensive pre-treatment diagnosis enhances the precision of targeted therapeutic interventions.
(2) Concerning the feeling of the patients
Scolioscan device can be operated without the need for a darkened room. During the examination, the room remains well-lit, creating a comfortable and secure environment for the patient. Additionally, its safety allows for repeated use during therapy.
(3) Unlimited scanning
Scoliosis assessment traditionally relies on X-ray examination, specifically measuring the Cobb angle from spine radiography. However, due to radiation exposure, repeated X-ray exam are not feasible, depriving patients of continuous monitoring. In contrast, the Scolioscan device employs ultrasound technology, enabling unlimited scanning without radiation risks.
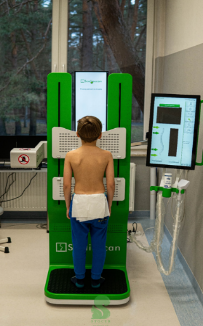

Figure 1. Examination of a child using Scolioscan device
Source: Mazowieckie Centrum Rehabilitacji STOCER